
October 2020
Summary
Cryptosporidium is a genus of parasitic protozoa that can cause cryptosporidiosis, a gastro-intestinal illness in humans, cattle and some other animals. In humans, it causes abdominal pain, watery diarrhoea, nausea, headaches and fever, but the infection is usually self-limiting and resolves within a few weeks. In immunocompromised patients, the infection can be more serious. It can become prolonged and rarely, fatal as a result of dehydration caused by chronic diarrhoea. These protozoa complete their life cycles in one host and their oocysts (spores) are highly infectious.
Cryptosporidiosis is primarily a waterborne disease, spread through the faecal-oral route. The oocysts can also be transmitted by handling infected animals, or person-to-person contact. The parasite can be found in soil, water or food and may be transmitted through surfaces that have been contaminated with the faeces of infected people or animals> Cryptosporidium requires a host in which to multiply and cannot grow in foods or water. The occurrence of large water- and foodborne outbreaks in several EU countries indicated that this parasite is widespread.
The majority of water treatment plants cannot completely guarantee removal of all Cryptosporidium oocysts from the water, since they are very small and resistant to chlorine (the disinfectant commonly used in these plants), so rendering much of the treatment process irrelevant.
Since the European Council Directive 98/83/EC on the quality of water intended for human consumption was brought in and transposed into UK legislation, they have had a beneficial impact on reported cases, as demonstrated by health surveillance data. The extent to which recreational waterways, such as lakes and private water supplies, continue to pose an occasional risk to health remains unclear, but other sources of contamination remain a cause for concern.
Cryptosporidium is inactivated by ultraviolet radiation (UV), heat, freezing and desiccation, hence heat-treated, frozen and dried foods should be safe, unless contaminated after processing.
Background
The protozoan parasite Cryptosporidium (Phylum apicomplexa, was described by Tyzzer in 1907, but its importance was only realised in the 1950s when the parasite was associated with diarrhoea in turkeys, and in the 1970s by veterinary workers investigating the cause of scours (severe and serious diarrhoea) in young farm animals[1]. Medically unimportant until the 1970s, Cryptosporidium was then recognised as a potential human pathogen when the first cases in humans were diagnosed in immunocompromised patients (a young child and an AIDS patient), reported in 1976 by Nime et al. and Miesel et al. In 1984, over 2000 people were affected with cryptosporidiosis during an outbreak in Braun Station, Texas, the first time Cryptosporidium was recognized as a waterborne pathogen. In the early 1980s, Cryptosporidium was first detected in Europe and was later identified as causing serious infections in severely immunocompromised patients, including patients with AIDS. Human cryptosporidiosis is now widely recognised as an endemic enteric pathogen, with illness in more than 90 countries and 6 continents, and it is one of the leading causes of human diarrhoeal disease. Infection rates are highest in developing countries and amongst children aged 1 to 5 years in developed countries. More than 1 million people have since been affected in documented outbreaks and the largest outbreak occurred in Milwaukee, Wisconsin in 1993[2] [3].
Cryptosporidium is an obligate parasite, i.e. it must have a host to complete its lifecycle. It is a very small protozoan belonging to the Coccidiasina (Coccidia)subclass which has emerged over the past decades as a major waterborne pathogen. While humans and livestock are the main sources of infection, it is found in a variety of vertebrate hosts including mammals, fish and birds. In humans it causes cryptosporidiosis, an intestinal infection, and it also infects many animal species, causing symptomatic illnesses and morbidity leading to significant economic losses [4].
At least eight Cryptosporidium species and two Cryptosporidium genotypes (cervine and monkey) have been found to infect humans, with over 90% [5] of human infections being due to Cryptosporidium hominis and Cryptosporidium parvum. The main species encountered in Europe, and particularly in the UK, is C. hominis, whereas in the Americas, Australia and Africa, C. parvum is the most identified genotype[6], although studies have shown a growing number of species can cause human disease[7]. C. hominis is probably specific to humans, with transmission via direct person to person contact through the faecal oral route due to poor hygiene. Two-thirds of cases are in young children (aged 1-5 years), and along with the elderly and other immunocompromised groups, are more at risk of severe disease, requiring hospitalisation. Many animal species can be infected with C. parvum and recent studies suggest that whether younger or older animals are infected may depend on the particular animal species), and transmission is via animals to humans, as well as between humans. Cryptosporidiosis can also be passed on as a secondary infection, as it requires a low infective dose of less than 100 organisms.
Infection, or illness, depends on several factors, based on the host, pathogen and environment, including the immune status of the host and the genotype of Cryptosporidium. The main site of cryptosporidiosis infection is the small intestine. Invasion of the host cells is restricted to the luminal border and leads to issue damage, which triggers the immunological and inflammatory responses of the host. Diarrhoea then occurs due to impaired intestinal absorption of fluids and nutrients, and the disruption in the normal ion flux.
Cryptosporidium parasites may also spread throughout the gastrointestinal and respiratory tracts, particularly in immunocompromised groups. Extra-gastrointestinal cryptosporidiosis has been reported in both immune-competent individuals and immunocompromised people including in the pancreas, liver and bile ducts. Respiratory involvement and sinusitis have been described in severe cases.
Oocysts are excreted in huge numbers and are capable of surviving for long periods in the environment, and whilst they can be found in soil, water or on food are most typically transferred through faecally contaminated water. Cryptosporidium may be more common in surface water than ground water because surface waters are more vulnerable to direct contamination from: fertiliser, sewage, industrial discharges, and runoff. Farmyard manure may contain high numbers of cryptosporidial oocysts and consequently water may be contaminated by manure or slurry, washed from fields into rivers, and vegetable crops may be contaminated by direct manuring of the fields in which they are grown. The management and storage of manure and slurry is an effective method of reducing infectivity, through raised temperatures and ammonia levels.
Cryptosporidium has been isolated from: fresh vegetables, irrigation water, contaminated drinking water, raw meat, fruit juices, unpasteurised milk and swimming pools.
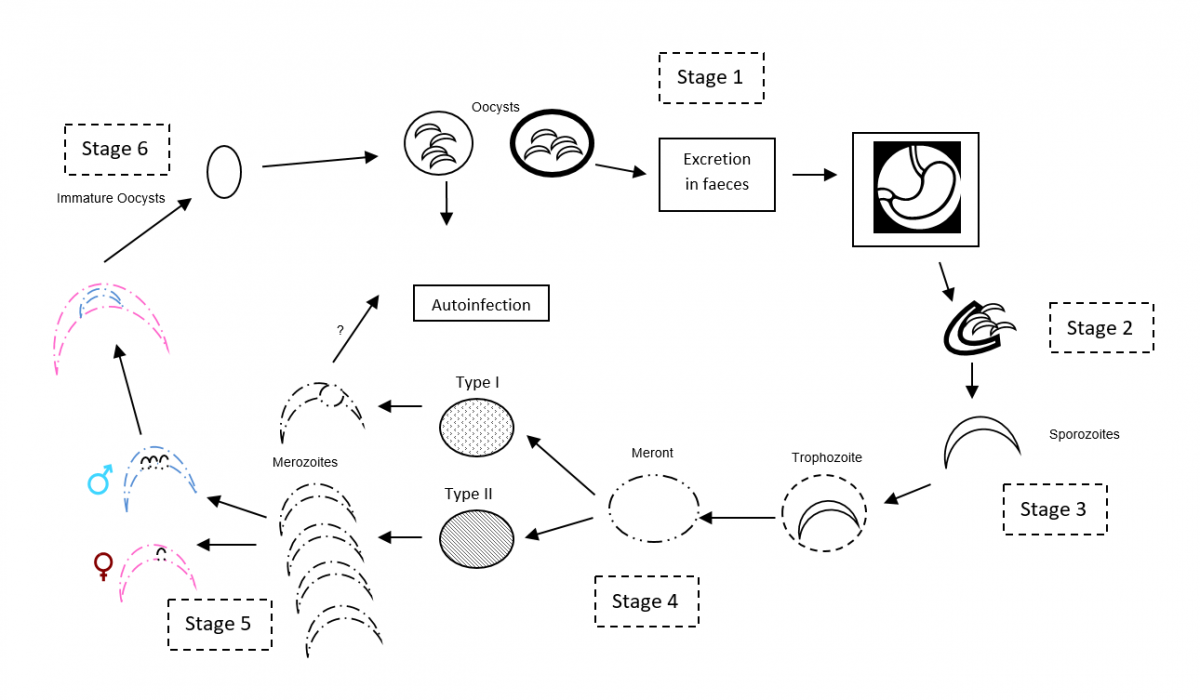
The lifecycle of Cryptosporidium is complex, and with the exception of one stage, is completed in a single vertebrate host in one to eight days. Cryptosporidium is excreted in the faeces of an infected host in the form of oocysts.
Oocysts are excreted by the host (stage 1 in Figure 1). Mature thick-walled oocysts are comprised of a trilaminate structure with a multilayered inner zone (which thin-walled oocysts lack), that maintains the viability of the sporozoites - the source of infection in their hosts. It is possible that there are two methods of infection: autoinfection may be possible in warm aqueous solutions, without exposure to pancreatic enzymes. Reinfection of the host occurs, possibly including sites outside of the intestine (e.g. testicles, eye conjunctiva, and respiratory tract), and the thick-walled oocyst, which has a high environmental resistance and is excreted in the faeces, where it can infect another host.
In stage 2, excystation (thinning of the oocyst wall) occurs, following ingestion by the host animal. The wall on either side of the suture, in the oocysts, retracts and coils inwards, following exposure to the stomach acid, bile salts and body temperature of the host. C. parvum and C. hominis oocysts release four motile sporozoites (motile, infective stage) into the small intestine.
The released slender, crescent-shaped sporozoites contain secretary apical organelles required for adhesion, penetration and inclusion in the host epithelial cells’ lining, the luminal surfaces of the digestive, and respiratory tracts. At the next stage (stage 3), as the sporozoites actively invade the cell wall, vacuoles form near the anterior end of the sporozoites and cluster together, surrounding the parasite and forming a parasitophorous vacuole, which fuses with the host’s cell membrane to form a host-parasitic interface. The sporozoites within are intracellular but are not directly in contact with the host cell cytoplasm (extracytoplastic). As this process progresses, the sporozoites becomes spherical, called trophozoites.
The asexual multiplication (metrogony, at stage 4) occurs when the trophozoite nucleus divides into meronts. Type I meronts develop nuclei which are incorporated into merozoites. In theory, each mature merozoite leaves the meronts to infect another host cell, developing into either type I or II meront. Type II meronts produce four merozoites. This is followed by a sexual reproduction stage (gamogony) where the type II meronts initiate sexual reproduction. The meronts differentiate into either male microgamonts (sperm equivalent) or female macrogamonts (ovum equivalent) (stage 5). Microgamonts become multinucleate, with each nucleus being incorporated into a microgamete. Macrogamonts remain uninucleate and become macrogametes. The microgametes then detect the microgametes by an unknown method and penetrate the membranes of both the host cell and macrogamete membrane.
The nucleus of the fertilised macrogamete develops into an oocyst (stage 6), in situ, by undergoing meiosis with four sporozoites developing. The oocysts are then either released into the intestinal tract, and excreted as faeces, or if they are in the respiratory tract, excreted in the respiratory or nasal secretions. They do not need any further maturation, unlike many other Coccidian protozoa.
The life cycle is repeated when sporulated oocysts (4 - 6 µm in diameter [8]) are excreted by an infected host, are subsequently ingested by a new host, and the sporozoites excyst within the small intestine [8].
Thick-walled oocysts are appreciably resistant to natural decay in the environment, as well as to most disinfection processes. They can remain viable for about 18 months in a cool, damp or wet environment, including seawater. They are quite common in rivers and lakes, especially where there has been sewage or animal contamination, and can survive for several months in standing water. Oocysts can survive for months in soil, and for up to a year in low-turbidity water. Oocysts appear to develop an enhanced impermeability to small molecules when in contact with faeces, which might increase the robustness of the oocysts when exposed to environmental pressures.[9]
Drying at ambient temperatures effectively reduces their infectivity. They are destroyed by freezing and are also heat sensitive. A temperature of 60°C inactivates oocysts in 5 - 10 minutes.
Oocysts are remarkably resistant to many common disinfectants, including chlorine-based compounds. Very high concentrations of most disinfectants may be effective, but such levels are not practical for water treatment due to cost and taste. This parasite is however susceptible to ozone and UV light.
Figure 1. Cryptosporidium lifecycle - simplified
Human cryptosporidiosis occurs in developed and developing countries, urban and rural areas, and in temperate as well as tropical climates. Infections have arisen from contaminated drinking water and food, swimming pools, and other recreational waters, daycare centres, and as a result of foreign travel.
The average incubation is 7 - 10 days (ranges from 1 to 28 days), with symptoms appearing 5 - 10 days after becoming infected by the ingestion of oocysts. Very low doses can initiate an infection, i.e. probably fewer than 100 oocysts.
The illness is characterised by profuse, watery diarrhoea, with abdominal pain. It can also cause vomiting, weight loss, loss of appetite, headache, fatigue, respiratory problems and a low-grade fever. Typically, the illness is self-limiting and resolves in 2 - 3 weeks, but it can last for up to 50 days. Only supportive treatment is available, and this will only be required in serious cases. However, in severely immunocompromised patients, such as AIDS sufferers, the infection may become chronic and serious, sometimes fatal. In these cases, other organs and tissues may become infected, including the biliary tract and respiratory system. Treatment options are still limited, and no fully effective drug treatment, or vaccine, is available for Cryptosporidium.
Mature oocysts are excreted in faeces in very high levels, during diarrhoeal illness, and are immediately infectious. Excretion may continue for some weeks after the cessation of diarrhoea.
As a contaminant of the water supply, the organism has the potential to infect large numbers of people, particularly where water supplies serve densely populated urban areas. It is this scale of potential harm that puts Cryptosporidium in the first league of emerging pathogens. As the oocysts can survive in cold, dark bodies of water and water supply pipes, it can strike a large number of people, and presents a threat to life for the elderly, the very young and immunocompromised.
The first identified waterborne outbreak in the UK was in Ayrshire in 1988 and affected 27 people [10]. This was followed in 1989 by a major outbreak affecting over 500 people in the Swindon area. Major outbreaks are rare, however many cases are thought to go unreported. Cryptosporidiosis may show a seasonal distribution; with swimming pool outbreaks continuing to occur, and incidences peaking in late summer and autumn, when swimming pool use is highest. Cryptosporidium is the most common enteric pathogen in children under 5 years of age. In one 2-year UK study, Cryptosporidium was found twice as often as Salmonella spp., in children aged 1 to 5 years. It is also recognised as a frequent cause of ‘traveller's diarrhoea’. Cases of Cryptosporidium infection associated with foreign travel increased on average by 4.6% each year between 2005 and 2014[11].
There have been a number of Cryptosporidium outbreaks in the United Kingdom:
West Sussex (April 2018)
This outbreak was associated with visits to a petting farm in April 2018 with14 cases confirmed [12]
Leeds (May 2016)
29 cases of cryptosporidiosis were confirmed by Public Health England (PHE) in people who had visited a petting farm in the area.
Bournemouth (2013)
An outbreak was linked to water supplies from the Alderney works with 29 confirmed cases, in a population of approximately 237,000 people served by the treatment works. C. hominis was detected in the water supply [13].
England and Scotland (May 2012)
A widespread foodborne outbreak of C. parvum occurred in May 2012, associated with the consumption of fresh pre-cut salad leaves. Over 300 cases were confirmed, in the then largest outbreak of foodborne cryptosporidiosis [14]. Although the precise source was not identified, infection was strongly associated with the consumption of mixed salad leaves sold by a single retailer, and typing revealed the outbreak strain to be C. parvum gp60 subtype IIaA15G2R1, a worldwide-distributed subtype highly prevalent in both livestock and humans.
Wales (August 2009)
Illness occurred in children and adults who swam at the Merthyr Tydfil Leisure Centre after Cryptosporidium oocysts were introduced into the swimming pool on Saturday 22nd August, late in the morning. The most likely cause was accidental smearing of faeces on a toddlers’ slide. A total of 106 cases of Cryptosporidium associated with this outbreak were identified, 45 of which were confirmed through laboratory testing [15].
Northamptonshire (June and July 2008)
23 cases of cryptosporidiosis, with the causative agent being confirmed as Cryptosporidium. cuniculus. The source was identified on 30th June 2008, from Cryptosporidium oocysts found in Pitsford Reservoir water. These were confirmed as being of the rabbit genotype C. cuniculus. Subsequently, a dead rabbit was found in a treated water tank at the water treatment works. The genotype of Cryptosporidium oocysts in the rabbit’s large bowel was indistinguishable from that of the oocysts found in the water [16].
Staffordshire (October 2007)
39 confirmed cases were identified with the most plausible explanation being that the infection was ingested in multiple swimming pools. One large swimming pool was the most frequently visited and was therefore considered a significant contributor to transmission, because of substandard filtration and maintenance systems. The 39 confirmed, and 18 probable, cases of cryptosporidiosis had a significant impact on the affected population and households, in terms of hospitalisation and absence from school or work [17].
North West Wales (2005)
Following 231 confirmed cases, environmental investigations, confirmed by microbiological testing, identified several routes by which C. hominis, from sewage treatment systems in the Cwellyn catchment, could have entered the reservoir, and subsequently the mains water supply from Llyn Cwellyn [18].
Grampian (January 2002)
The overall conclusion was that the outbreak of cryptosporidium was caused by the contamination of drinking water supplied from the Invercannie Treatment Works, due to a reduction in the effectiveness in the slow sand filtration system. There were 143 cases [19].
Research undertaken by Chalmers et al (2019) [20], analysed data associated with human outbreaks of Cryptosporidium in England and Wales, from 2009 to 2017. A total of 178 outbreaks, involving 4031 laboratory confirmed cases, were identified. The infecting Cryptosporidium sp. was identified in 74% (131) of outbreaks: 69 were C. parvum, 60 C. hominis, and 2 outbreaks cases were infected with either species. Animal contact, environmental contact, and food-borne outbreaks were exclusively C. parvum and were mainly in the first half of the year. Recreational water outbreaks were predominantly C. hominis and were mainly in the second half of the year. Outbreaks attributed to person-to-person spread were exclusively C. hominis, and all occurred in October. Both C. parvum and C. hominis caused drinking waterborne outbreaks.
Although Cryptosporidium is resistant to chlorine, the multi-barrier approach to water treatment adopted by the industry includes effective barriers to the organism.
It is unclear how the oocysts are able to survive chlorination, although it is believed that its protective 'oocyst' membrane plays a role. One theory is that the organism might use a pump mechanism to expel toxins from its inside before they cause the oocyst harm. Whatever its defence, it is effective as a study by the US Environmental Protection Agency suggested that Cryptosporidium could even live on chlorine products.
Although difficult to detect, it is still relatively rare in most well-maintained public water systems, with the greatest danger being to those people who use private water supplies (as these supplies are tested). Research in the United Kingdom suggests effective screening requires very frequent analysis of large volumes of water samples. Private wells are typically less advanced than those of water treatment plants, meaning the protozoa is able to pass easily, often escaping detection by hiding in the biofilm of the water system.
In the UK, water companies adopt a formal risk-based approach to assessing and managing Cryptosporidium and any other substance that could constitute a potential danger to human health. Companies carry out routine monitoring of treated water, and on the rare occasions where Cryptosporidium is detected in the treated water, companies immediately investigate the cause and make corrections, while consulting with local health protection units to determine measures needed to protect public health.
The complete removal of Cryptosporidium oocysts from water supplies is difficult to achieve in conventional water treatment plants. The oocysts are resistant to normal chlorine disinfection treatment and, as they are very small (4 - 6 μm in diameter), some pass through the flocculation and sand filtration systems. Control measures may be different in supplies from bore holes as compared to those derived from surface waters, although even those from bore holes may be susceptible to oocyst contamination. Sources derived from surface water will inevitably be susceptible to runoff from land contaminated by animals as well as, on occasion, human sewage. Modern drinking water treatment combines a multi-barrier approach of good maintenance and design of the filtration systems with UVC, ozone or ultrafiltration as a tertiary treatment, to inactivate protozoan oocysts. Careful control of the treatment facility and processes, especially during back-flushing to clear the filtration beds [8], is essential. In practice, many conventional water treatment plants cannot guarantee the complete removal of these protozoa from water supplies. The fairly high operating costs, and inability to deal with seasonal fluctuations in pathogen load, reinforces the need to investigate new water treatment technologies and control strategies [21].
In view of this, both English and American public health authorities have advised severely immunocompromised people to boil drinking water, in order to reduce the chance of acquiring waterborne cryptosporidiosis. It is sufficient simply to bring water to the boil to eliminate Cryptosporidium. It should be stressed that, in order to be effective, the guidance must be followed consistently for all water used for drinking, or for washing foods intended for consumption without cooking. It should also be noted that bottled water is not guaranteed free from Cryptosporidium.
Whilst rare, there have been outbreaks of water-borne cryptosporidiosis in both the UK and the US and these have generally been shown to be caused by inadequate water treatment, or by breaches of the integrity of distribution systems. Increased understanding of Cryptosporidium contamination, and the considerable amounts of monitoring data that are now available, have helped water suppliers to establish effective means of controlling Cryptosporidium in drinking water. However, there is a need for constant vigilance. A report by the independent Drinking Water Inspectorate (DWI) found that the quality of drinking water remained exceptionally high in 2018. Around four million samples were taken in England and Wales, with 99.96% meeting, or exceeding, the standards set by the DWI [22].
Interestingly, one study in Scotland suggested that while oocyst removal from drinking water supplies decreased the risk of waterborne cryptosporidiosis, the reduction in circulating antibody response may indicate decreased protective immunity, and that the population may therefore be at increased infection risk from exposure to other sources. [23]
Cryptosporidium cannot grow in food; however, oocysts will survive in wet or moist foods if they become contaminated. Foodborne outbreaks of cryptosporidiosis have been recently documented in several EU countries. Implicated foods include fresh produce and unpasteurised, or inadequately pasteurised milk. Globally, Cryptosporidium is responsible for more than 8 million cases of foodborne illness annually [24].
Of particular importance is the outbreak in May 2012 that occurred in England and Scotland, [14] which is the largest documented outbreak of cryptosporidiosis attributed to a food vehicle, with more than 300 cases involved. There was also an outbreak in Finland in 2012, associated with the consumption of frisée salad [25]. Traceback investigations revealed the source of the salad to be an outdoor grower in the Netherlands, where there had been heavy rainfall during the growing season.
Raw milk, raw sausages and offal, together with fruit, vegetables, salad products and filter feeding shellfish are at risk if in contact with manure, sewage or contaminated water, and therefore may become contaminated. Cooked foods are not thought to be a risk since the normal recommended time and temperature for controlling bacterial food poisoning (cooking to an internal temperature of 70°C for 2 minutes) will probably inactivate Cryptosporidium. Heat processed foods have never been shown to be a source of infection and studies show standards thermal treatments are effective. Oocysts will not survive freezing.
There is a potential danger that infected food handlers could contaminate food. UK guidance states that food handlers, and carers of highly susceptible patients, should be excluded from work until diarrhoea has stopped [26]. Cases should avoid using swimming pools for two weeks after the first normal stool because shedding of oocysts can continue after diarrhoea has stopped. People with symptoms must not handle foods, and advice should be taken on when they can restart such work (usually at least 48 hours after symptoms resolve). Personal hygiene is very important with this illness, because the infective dose is so low.
Unlike most bacterial enteric pathogens, Cryptosporidium is difficult to detect. It is not possible to grow Cryptosporidium routinely in foods, or beverages, to levels where they may be readily detected, hence examination of foods for this protozoan has in the past been considered impractical.
Techniques for sampling and analysis are complicated and time-consuming, requiring the filtration of large volumes of water (100 - 1000 litres), followed by several stages of elution, isolation and concentration of the oocysts, and then identification and enumeration. Organisms in water samples can be concentrated by filtration and by immunomagnetic separation. Deposits are then usually examined by microscopy, with differential staining techniques being available to distinguish viable from non-viable oocysts. Immunoassays and PCR-based procedures are also used.
Initial testing does not provide information on whether the oocysts are viable and therefore capable of causing disease, this requires further testing. Identification of the species sub-type can be helpful in tracing the source of contamination - this requires much additional work.
- Agriculture
Farm management practices to reduce the occurrence of Cryptosporidium:
- Feeding practices that promote good hygiene including the use soap/detergent when washing bottles and feeding equipment.
- Housing practices that promote good hygiene to prevent infection of animals.
- Reducing infection by steam cleaning of equipment where possible/practice (oocysts are inactivated above 65°C).
- Isolating ill animals.
- Sanitary disposal of animal manure. Flies are strongly attracted to animal manure and may be carriers of oocysts in their exoskeleton and digestive tracts [27).
- Optimise management and storage of manure and slurry to reduce the infectivity of oocysts through raised temperature and ammonia levels.
- Reduce runoff from animal farms into drinking water supplies, for example by planting strips of grass or vegetation. This may help to trap sediment and therefore reduce the organic matter contamination.
- Processing (including water suppliers, industries that use fresh product, and operations where contaminated process or wastewater could be used)
- All water that is to be used in direct contact with food and food contact surfaces must be of potable quality and should be free of pathogenic microorganisms
- A consistent supply of food-safe water for use in direct contact with foods and food contact surfaces is required
- Treatments for bottled, natural mineral waters and spring waters that are effective in reducing Cryptosporidium include physical removal (filtration or decanting), the addition or removal of carbon dioxide, and treatment with ozone. A multi-barrier approach is the most effective in reducing or eliminating Cryptosporidium oocysts
- When water to be used for drinking, bottling or vending can be treated prior to use, microfiltration membranes, or similar, can be incorporated in conjunction with other measures (such as UV treatment, reverse osmosis or pasteurisation/distillation) to reduce further the likelihood of Cryptosporidium contamination
- Water to be used as an ingredient (e.g. for juices and beer), or in the production of baby formula, should be filtered with/without other treatment systems
- A risk management approach, such as HACCP, should be utilised, and Cryptosporidium included in the assessment when assessing the risk and requirement/decision on the technologies to be used, taking into account:
- water source
- pH (natural acidity, carbonation)
- temperature of product
- presence of preservatives
- final consumer
- whether chemical technologies are sufficient, or physical removal methods are required
|
1 |
Manual of Diagnostic Tests and Vaccines for Terrestrial Animals 2010, OIE. http://www.cabi.org/ahpc/default.aspx?site=160&page=3323 |
|
2 |
Environmental Protection Office of Water March 2001, Cryptosporidium: Drinking Water Health Advisory |
|
3 |
Cryptosporidium species a "new" human pathogen. D P Casemore, R L Sands, A Curry, J Clin Pathol 1985;38:1321-1336 doi:10.1136/jcp.38.12.1321 |
|
4 |
Enteric Protozoa: Giardia and Cryptosporidium. Prepared by the Federal-Provincial-Territorial Committee on Drinking Water. http://www.hc-sc.gc.ca/ewh-semt/consult/_2010/giardia- cryptosporidium/draft-ebauche-eng.php#ii |
|
5 |
Rev Argent Microbiol. 2009 Jun-Sep; 41(3):185-96. Cryptosporidiosis: an emerging zoonosis. Del Coco VF, Córdoba MA, Basualdo JA |
|
6 |
Microbes Infect. 2004 Jul;6(8):773-85. A review of the biology and epidemiology of cryptosporidiosis in humans and animals. Ramirez NE, Ward LA, Sreevatsan S |
|
7 |
Cryptosporidiosis: A report on the surveillance and epidemiology of Cryptosporidium infection in England and Wales, Gordon Nichols et al. |
|
8 |
Cryptosporidium and Cryptosporidiosis, Second Edition, edited by Ronald Fayer, Lihua Xiao, ISBN-10: 1420052268 |
|
9
|
Appl. Environ. Microbiol. November 1992 vol. 58 no. 11 3494-3500 Survival of Cryptosporidium parvum oocysts under various environmental pressures. L J Robertson, A T Campbell and H V Smith |
|
10 |
An outbreak of waterborne cryptosporidiosis caused by post-treatment contamination, H. V. Smith et al, J of Epidemiology and Infection, vol. 103, 1989 |
|
11
|
Travel-associated Cryptosporidium infection in England, Wales and Northern Ireland: 2014. Public Health England |
|
12
|
Public Health England warning over diarrhoea illness linked to West Sussex farm visits. https://www.chichester.gov.uk/article/29968/Public-Health-England-warning-over-diarrhoea-illness-linked-to-West-Sussex-farm-visits |
|
13 |
Sembcorp fined over unfit tap water in Bournemouth. https://www.bbc.co.uk/news/uk-england-dorset-32056407 |
|
14 |
An outbreak of Cryptosporidium parvum across England & Scotland associated with consumption of fresh pre-cut salad leaves, May 2012. C McKerr et al PLoS One. 2015;10(5):e0125955. Published 27 May 2015 |
|
15 |
Outbreak of Cryptosporidium infection in a swimming pool complex in Merthyr Tydfil South Wales. https://www.nric.org.uk/node/53471 |
|
16 |
The first recorded outbreak of cryptosporidiosis due to Cryptosporidium cuniculus (formerly rabbit genotype) following a water quality incident. RL Puleston et al (2014) Journal of Water and Health 12.1 |
|
17 |
http://www.eurosurveillance.org/images/dynamic/EE/V13N45/art19028.pdf |
|
18 |
http://www.anglesey.gov.uk/upload/public/attachments/51/cryptosporidiumenglish.pdf |
|
19 |
http://www.nhsgrampian.org/grampianfoi/files/CryptoAberdFRep2002.pdf |
|
20 |
Analysis of the Cryptosporidium spp. and gp60subtypes linked to human outbreaks of cryptosporidiosis in England and Wales, 2009 to 2017. Parasites & Vectors volume 12, Article number: 95 (2019) |
|
21 |
Photocatalytic inactivation of Cryptosporidium parvum on nanostructured titanium dioxide films. (2010) O. Sunnotel, R. Verdoold, P. S. M. Dunlop, W. J. Snelling, C. J. Lowery, J. S. G. Dooley, J. E. Moore and J. A. Byrne. J Water Health 2010 Mar; 8(1):83-91 |
|
22 |
Drinking Water Inspectorate (DWI) Drinking Water 2018 http://www.dwi.gov.uk/about/annual-report/2018/index.html |
|
23 |
Effects of drinking-water filtration on Cryptosporidium seroepidemiology, Scotland. Ramsay, CN; et al Emerging Infectious Diseases (Emerg Infect Dis), 20 (2014), pp 70 – 76 |
|
24 |
Foodborne cryptosporidiosis Ryan, U; Hijjawai, N; Xiao, L. International Journal for Parasitology Volume 48, Issue 1, January 2018, Pages 1-12 |
|
25 |
Åberg R, Sjöman M, Hemminki K, Pirnes A, Räsänen S, Kalanti A, et al. Cryptosporidium parvum caused a large outbreak linked to frisée salad in Finland, 2012. Zoon Public Health 2015; 62:618–24 |
|
26 |
Working Group of the former PHLS Advisory Committee on Gastrointestinal Infections. Preventing person-to-person spread following gastrointestinal infections: guidelines for public health physicians and environmental health officers. Communicable Disease and Public Health (Commun Dis Public Health) 2004;7:362–84 |
|
27 |
Chin James. Control of Communicable Diseases Manual. 17th Ed, 2000; American Public Health Association |
|
|
Summary Lake IR, Nichols G, Bentham G, Harrison FCD, Hunter PR, Kovats RS. Cryptosporidiosis decline after regulation, England and Wales, 1989–2005. Emerg Infect Dis April 2007 http://wwwnc.cdc.gov/eid/article/13/4/06-0890.htm
|
Institute of Food Science & Technology has authorised the publication of the following updated Information Statement on Cryptosporidium, prepared by Julie Ashmore CSci FIFST, peer-reviewed by professional members of IFST and approved by the IFST Scientific Committee.
This information statement is dated October 2020, replacing that of December 2013.
The Institute takes every possible care in compiling, preparing and issuing the information contained in IFST Information Statements, but can accept no liability whatsoever in connection with them. Nothing in them should be construed as absolving anyone from complying with legal requirements. They are provided for general information and guidance and to express expert professional interpretation and opinion, on important food-related issues.